Should dolutegravir always be withheld in people with HIV on ... - BMC Infectious Diseases
This 44-year-old man was enrolled in a prospective cohort study (GLucose Metabolism changes in Ugandan HIV patients on Dolutegravir, GLUMED study) evaluating glucose metabolism changes in anti-retroviral therapy (ART) naïve PWH on tenofovir/ lamivudine/ DTG (TDF/3TC/ DTG) for 48 weeks [13]. PWH with normal 2-hour oral glucose tolerance tests (OGTTs) were enrolled for 48-week follow up with serial OGTTs at 12 and 36 weeks. The primary aim of the study was to determine incidence of T2DM in Ugandan PWH on DTG and describe glucose metabolism changes in patients with incident hyperglycemia versus those without.
Baseline evaluation
At enrollment on ART, he reported no other known chronic illnesses and long-term medication. He was not severely immunocompromised with a baseline CD4 + cell count of 261cells/mm3 and was in WHO clinical stage I. Baseline viral load was not done. He had a normal baseline OGTT with fasting blood glucose (FBG)- 88.2 mg/dl and 2-hour blood glucose (2hBG) of 153 mg/dl and normal blood pressure. He did not have conventional risk factors for diabetes like family history of T2DM, obesity (body mass index (BMI) of 17.5 kg/m2)), anti- glutamic acid decarboxylase (anti-GAD) antibodies and insulin resistance (HOMA IR − 0.6 (normal < 2). He was a builder with calculated WHO metabolic equivalent minutes of 4800 per week on average (met the WHO recommended physical exercise recommendations for good physical health) [14]. However, he was positive for anti- Islet cell antigen 2 (anti-IA2) antibody (which is more predictive of type 1 DM) and had reduced pancreatic beta cell function (HOMA% β- 68% (normal = 100%)). Insulin resistance and pancreatic beta cell function was calculated using homeostatic modelling, a factor of serum fasting glucose and fasting insulin.
Diagnosis of T2DM
During the 36-week study visit, he was diagnosed with T2DM basing on a 2hBG of 259 mg/dl. His BMI had increased to 20.9. Other tests included: HBA1C- 4.2%, HOMA IR- 2, HOMA% β- 101.4%. DTG was substituted with efavirenz according to the Uganda HIV treatment guidelines that recommended mandatory substitution of DTG in case of incident T2DM [9].
Follow up after T2DM diagnosis and withholding of DTG
He was managed on a low carbohydrate diet without T2DM pharmacologic intervention. Serial blood glucose evaluations at 2,4, 8, 12 and 24-weeks post T2DM diagnosis were within normal ranges. At 24 weeks, his HBA1C had increased to 4.9%. Insulin resistance continued to worsen with a HOMA IR of 3.5% while his pancreatic beta cell function continued to increase with HOMA %β = 134.9%. Dietary non-pharmacological management was continued after 24 weeks. Changes in BMI, blood glucose, HBA1C, HOMA IR and HOMA % β have been summarized in Figs. 1, 2 and 3.
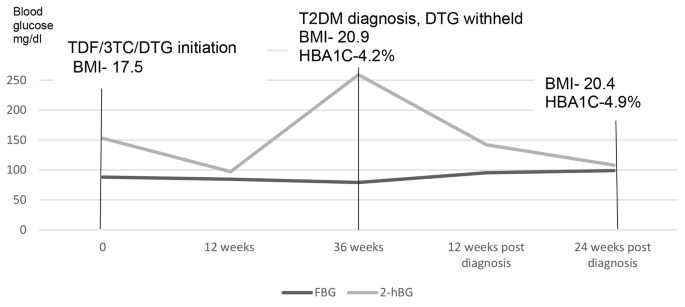
Changes in fasting and 2-hour blood glucose before and after withholding dolutegravir
TDF/3TC/DTG- tenofovir/ lamivudine/ dolutegravir, BMI- body Mass Index, T2DM-Type 2 Diabetes Mellitus, HBA1C- glycated hemoglobin
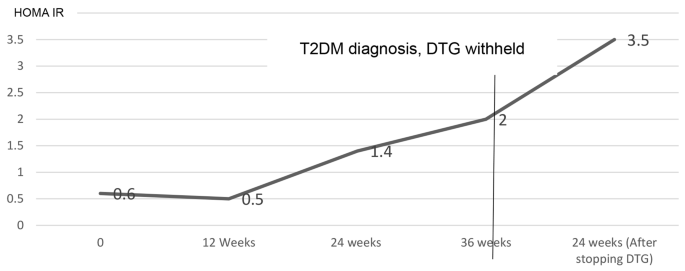
Changes in insulin resistance calculated by Homeostatic modelling (HOMA IR) before and after withholding dolutegravir
HOMA IR- homeostatic model of insulin resistance, DTG- dolutegravir, T2DM-Type 2 Diabetes Mellitus

Changes in pancreatic beta cell function calculated by Homeostatic modelling (HOMA %β) before and after with-holding dolutegravir
HOMA %β- Homeostatic model of pancreatic beta cell function, DTG- Dolutegravir, T2DM-Type 2 Diabetes Mellitus. (HOMA %β at baseline and 12 weeks was not calculated because the serum insulin was less than the HOMA calculator threshold)
Comments
Post a Comment